피부염의 원인균인 황색포도상구균 내성 균주(MRSA)에 대한 에센셜 오일의 항균 효과
Antibacterial Effect of Essential Oil on Staphylococcus Aureus-resistant Strain (MRSA), the Causative Agent of Dermatitis
Article information
Trans Abstract
The emergence of multidrug-resistant microorganisms represents a global challenge owing to the lack of new effective antimicrobial agents. Essential oils could be an alternative to antibiotics because of their anti-inflammatory, antiviral, antibacterial, and antibiofilm activities. Therefore, this study aimed to investigate the antibacterial activity of essential oils as an alternative to antibiotics. In the present study, we cultured methicillin-resistant Staphylococcus aureus (MRSA) with two concentrations (0.5% and 1.0%) of 17 types of essential oils and the antibiotic oxacillin as the control. The optical density of the culture suspensions at 600 nm was determined to assess the effect of the essential oils on MRSA. At 0.5% concentration, 8 essential oils demonstrated higher antibacterial activity than oxacillin, with palmarosa, melissa true, and rose geranium showing the highest antibacterial activity. At 1% concentration, 13 essential oils showed higher antibacterial activity than oxacillin, with melissa true, palmarosa, lemongrass, and rosemary verbenone showing the highest antibacterial activity. Furthermore, essential oils isolated from leaves showed higher antibacterial ability. Overall, the antibacterial activity of essential oils against MRSA varied with the concentration, type, and extraction site. Therefore, our study provides a basis for the selection and use of essential oils for antibacterial activity against MRSA.
I. Introduction
Staphylococcus aureus is one of the most common foodborne pathogens that can invade the body and cause a wide range of diseases, such as skin infections and food poisoning (Laupland et al., 2003). It has also been shown to be associated with atopy (Geoghegan et al., 2018; Tian et al., 2021). Since the discovery of the first cases of drug-resistant microbial strains in 1961, the prevalence of lethal methicillin-resistant Staphylococcus aureus (MRSA) has markedly increased worldwide (Bertrand, 2010). Chronic cutaneous wound infections associated with methicillin-resistant Staphylococcus aureus (MRSA) pose a great challenge owing to the difficulties in eradicating MRSA from the wound site. MRSA has developed multiple mechanisms to develop resistance against all conventional antibiotics (Van Bambeke et al., 2008). Additionally, recent investigations indicate that at least 65% of all diseases caused by bacterial infections and 70% of chronic infections in humans may be biofilm related (Fastenberg et al., 2016; Potera, 1999). Bacteria in biofilms are much more resistant to antibiotics than bacteria alone; for this reason, it is necessary to identify and develop new antibacterial agents for inhibiting or eradicating the formation of bacterial biofilms (Gómez-Sequeda et al., 2020).
Vegetable fatty acids and essential oils are prepared by various extraction methods. Not only aromatherapy, but also antiseptic effect and useful healing properties It has the power to be used in various fields including skin (Lee et al., 2012). Essential oils are used in various industries such as cosmetics, food flavorings, and pesticides, as well as medicines for disease treatment, cosmetic massage, cosmetics, and air fresheners. Essential oils have a high lipid content, so they are quickly distributed in the body, resulting in rapid drug effect and few side effects (Kim et al., 2018). Furthermore, since essential oils are mainly composed of aldehydes, phenols, and terpene alcohols that are associated with high antibacterial activity (Bassolé & Juliani, 2012), they may also constitute as bactericidal, fungicidal, anthelmintic, and insecticidal sources (Ambrosio et al., 2017; Bazargani & Rohloff, 2016). The Food and Drug Administration considers many individual components of essential oils to be safe. Therefore, they can be used for multiple applications in the cosmetic, medical, pharmaceutical, food, and health industries (Bakkali et al., 2008; Swamy et al., 2016).
The present study aimed to investigate the antibacterial activity of essential oils as an alternative to antibiotics, which may prevent the increasing microbial resistance due to the excessive use of antibiotics. This study conducted an antibacterial test by randomly selecting 17 types of well-known oils so that essential oils can be used in various practical applications. The results of this study can serve as a basis for the selection and use of essential oils with antibacterial ability in MRSA to reduce the abuse of antibiotics and better prevent antibiotic resistance.
II. Materials and Methods
1. Materials
In the present study, we used the MRSA strain ATCC 33591, purchased from the American Type Culture Collection, and 17 kinds of essential oils were randomly selected from the products supplied by the Korean Aromatherapy Certification Society. The essential oils were classified according to the plant extraction site and type (Table 1). The standard amount of Oxacillin (Sigma-Aldrich, Steinheim, Germany) antibiotic was used as a control. A FlexStation 3 Multi-Mode Microplate Reader (Molecular Devices, San Jose, CA, USA) was used to measure absorbance.

Classification of the 17 essential oils by type and plant extraction site
2. Bacterial culture
MRSA was cultured on a nutrient agar plate (MB-N1036, KisanBio, Seoul, Korea). The cultured cells were suspended at a volume ratio of 1 × 106 according to the 0.5 MacFarland standard using nutrient broth (Difco, Le Pont-de-Claix, France). After dispensing 100 μl of the bacterial suspension into a 96-well plate, 100 μl of essential oils (1% and 0.5% concentrations) or 100 μl of oxacillin (CLSI standard concentration; 2 μg/ml) were added 3 each wells, and the plate was then incubated at 37°C for 18 h in an incubator (Fig. 1). The essential oil concentrations of 1% and 0.5% were diluted using the nutrient broth (Difco, Le Pont-deClaix, France). The essential oil diluent was homogenized by voltexing for at least 1 minute to properly mix with the medium. And pipeting was done at medium depth.
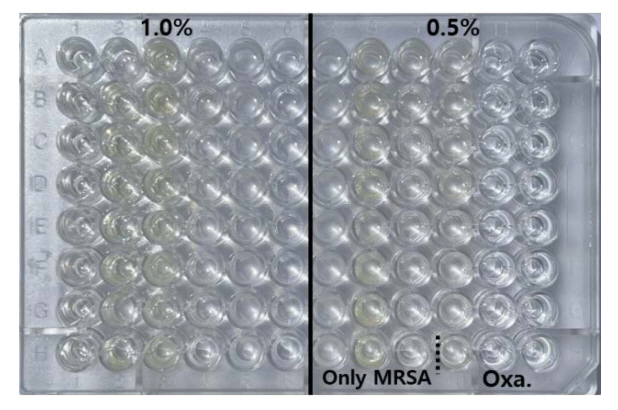
MRSA antibacterial test result image. MRSA was suspended in NB medium at a volume ratio of 1×106 according to 0.5 MacFarland standard, and 100 μl was dispensed, and essential oil and oxacillin (CLSI standard concentration; 2 μg/ml) adjusted to concentrations of 0.5% and 1.0% were added to 3 wells. 100 μl aliquots were added and the plates were incubated in an incubator at 37°C for 18 h.
3. Cell concentration detection
Optical density (OD) was measured at 600 nm as an endpoint using the spectrophotometer absorption program of the FlexStation 3 Multi-Mode Microplate Reader (V3.4.4.2413; Molecular Devices, California, USA). Three replicates were performed to improve accuracy.
4. Statistical analysis
For statistics, IBM SPSS Statistics 20 (IBM Corp., NY, USA) program was used, and a one-way ANOVA test was performed to verify the statistical significance between the control group and the experimental group. And the significance test was performed at the level of *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001; #P < 0.05, ##P < 0.01, ###P < 0.001, ####P < 0.0001. * = Significance compared to control, # = Significance compared to Oxacillin. This experiment was repeated three times.
III. Results
After reading each essential oil with a wavelength of 600 nm in a micro plate reader, the inhibition rate is shown in Table 2 and Figure 1, 2 by comparing the resulting value with the Control. First, compared to the control (100%), the inhibition rate of oxacillin was 72%. being OXA one of the more active beta-lactam against S. aureus but to which MRSA is typically resistant (David & Daum).

Evaluation of the antibacterial ability of the 17 essential oils by concentration
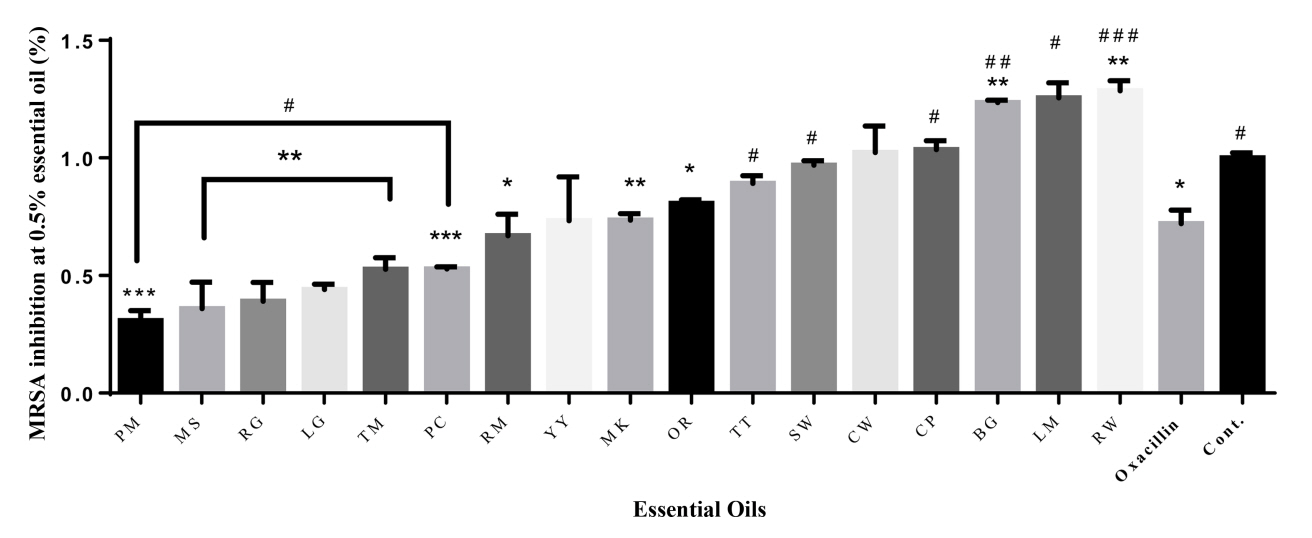
Comparison of antibacterial activity by concentration of the 17 essential oils (0.5%) against methicillin-resistant Staphylococcus aureus strain ATCC 33591. The antibacterial activities of the essential oils are arranged in ascending order from left to right. * = Significance compared to control, # = Significance compared to Oxacillin *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001; #P < 0.05, ##P < 0.01, ###P < 0.001, ####P < 0.0001
Palmarosa (31%), Melissa True (36%), Rose Geranium (39%), Lemongrass (44%), Patchouli (53%), Thyme (53%), Rosemary Verbenon (67%) at 0.5% Concentration showed higher antibacterial activity than oxacillin (72%). In particular, Palmarosa (31%), Melissa True (36%), and Rose Geranium (39%) showed the highest antibacterial activity. The inhibition rates observed in ylang-ylang and manuka were 73% and 74%, respectively, showing the same inhibition rate as oxacillin. However, the remaining four essential oils had lower antibacterial activity than oxacillin.
At 1.0% concentration, melissa true (24%), palmarosa (27%), Lemongrass (28%), rosemary verbenone (29%), rose geranium (47%), pachuli (56%), orange (57%), Thyme (62%), ylang ylang (65%), manuka (67%), and cedarwood atlas (68%) had higher antimicrobial activity than oxacillin (72%), melissa true (24%), palmarosa (27%), Lemongrass (28%) had the highest antibacterial activity. Tea tree (74%) had similar values for oxacillin. However, the rest of the essential oils had lower antibacterial activity than oxacillin. In the case of lemon and bergamot, the bacteria were more active.
To verify the significance of the following results, one-way ANOVA analysis was performed. The part showing significance at 0.5% compared to Control was marked with *. Palmarosa and patchouli showed the highest significance, and all oils except ylang-ylang, tea tree, sandalwood, cedarwood, cypress and lemon showed significance. At 1.0%, almost all essential oils showed high significance, and lemon and bergamot showed no significance. The portion showing significance at 0.5% compared to oxacillin was marked with #. Rosewood and bergamot showed the highest significance, and all oils except rosemary, ylang-ylang, manuka, orange and cedarwood showed significance. At 1.0%, significance was shown in the remaining essential oils except for thyme, ylang-ylang, manuka, cedarwood, tea tree, and rosewood.
In general, essential oils isolated from leaves showed higher antimicrobial activity than those isolated from other plant parts.
IV. Discussion
Recently, as many clinical results on side effects and toxicity of synthetic drugs are frequently reported, research for the development of a new type of functional cosmetic material that is safe from natural products is in progress (Kim et al., 2009) Essential oil is a complex of aromatic substances extracted from plants by methods such as compression or distillation and having a unique fragrance depending on the species, part, and production area (Ha, 2000). Various physiological activities and effects such as antioxidant, antibacterial, blood circulation improvement, and stress reduction have been reported, and it is being utilized in various industries such as cosmetics, food, and pharmaceuticals (Jeong & Park, 2012). with a special focus on essential oils. Essential oils are naturally extracted from different parts of aromatic plants and possess a complex chemical composition that can be a potential source of new antibacterial compounds (Orchard & van Vuuren, 2017; Tariq et al., 2019). The purpose of our study was to evaluate the antibacterial ability of 17 essential oils at concentrations of 0.5% and 1.0% by determining their antibacterial effects on MRSA. Hu et al, 2019 showed that Litsea cubeba essential oil effectively inhibits MRSA without affecting its cytotoxicity. Additionally, Oliveira Ribeiro et al., 2020 showed that oregano, clove, palmarosa, and lemongrass had strong antibacterial abilities against MRSA. Similarly, the present study showed that palmarosa and lemongrass had high antibacterial activity against MRSA. Melissa true demonstrated higher antimicrobial activity than penicillin (Mimica-Dukic N. et al., 2004) against various pathogens, such as Staphylococcus aureus and Escherichia coli, and to have lower antimicrobial activity against Pseudomonas aeruginosa (Kwon et al., 2017). Similarly, in the present study, the antibacterial activity of melissa true was observed to be higher than that of oxacillin against MRSA. Chao et al., 2008 found that 78 of 91 single essential oils exhibited inhibitory zones against MRSA, with lemongrass, cinnamon, and melissa true essential oils having the highest levels. Comparably, in the present study, lemongrass and melissa true showed high antibacterial activity against MRSA. Considering the overall antibacterial activity observed in the present study, it seems that essential oils extracted from leaves have a high antibacterial effect. Previous studies have shown similar results (Oliveira Ribeiro et al., 2020; Chao et al., 2008). In contrast, bergamot and rosewood showed low antibacterial activity against MRSA. In a previous study (Chao et al., 2008), our results were the same, but in another study (Salem et al., 2017), citrus essential oils, such as bergamot and lemongrass, showed high antibacterial activity against MRSA. Collectively, it can be inferred from the present study and previous studies that the antibacterial efficacy of essential oils depends on their type, concentration and extraction site.
The present study had several limitations. Antibiotics, such as vancomycin, which are widely used for the treatment of MRSA in clinical practice, were not used. Future research should use antibiotics that have antibacterial activity against resistant strains, such as vancomycin. Furthermore, there was a lack of comparison with different concentrations and diversity of essential oils. Therefore, various essential oils with several concentrations are required for improved antibacterial testing.
Nevertheless, our study showed the antibacterial ability of 14 different types of essential oils compared to oxacillin. Since the antibacterial activity against MRSA differs depending on the essential oil concentration, type, and extraction site, the essential oil concentration can be adjusted according to each individual. Therefore, the present study provides a basis for the selection and use of essential oils for antibacterial activity against MRSA.

Comparison of antibacterial activity by concentration of the 17 essential oils (1.0%) against methicillin-resistant Staphylococcus aureusstrain ATCC 33591. The antibacterial activities of the essential oils are arranged in ascending order from left to right. * = Significance compared to control, # = Significance compared to Oxacillin *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001; #P < 0.05, ##P < 0.01, ###P < 0.001, ####P < 0.0001