한의원의 비만 치료 및 비만 관리 행태 조사 분석
Investigation and Analysis of Obesity Treatment and Obesity Management Behavior in Korean Medicine Clinics
Article information
Trans Abstract
After the completion of obesity treatment, customer (patient) satisfaction was high, and it was found that if obesity treatment was added to the existing treatment at Korean medicine clinics, sales would increase. And the respondents answered that if obesity management is implemented, sales seem to be increased at a high rate. If providing information on effective obesity management methods that have been verified in the beauty field to Korean medicine doctors, a high proportion of them were willing to combine the current obesity treatment with cosmetic therapy, and also responded that the possibility of mutual fusion and collaboration in the future is high. There were many positive answers about whether or not obesity management at korean medicine clinics would contribute to opportunities for field training and employment for students enrolled in the beauty field. Also, if obesity treatment and obesity management are mutually fused or collaborated, they also showed a high positive rate on whether they think the sales of the beauty industry and the Korean medicine medical tourism industry will increase. A high percentage of responses also showed that if obesity treatment and obesity management were mutually fused or collaborated, it would help to increase the preference and vitalization of the Korean medicine medical industry and beauty tourism industry by domestic and foreign tourists.
I. 서 론
독일 철학자 바움가르텐(Baumgarten)이 처음 사용한 에스테틱(Aesthetica)은 미(美; 아름다움)를 논하는 의미이고, 칸트(Kant)와 장자의 미 개념 연구에서는 미를 자유로 규정하고 인간 삶의 의미만큼이나 포괄적이고 전체적이며 유동적인 개념이라고 하였다(Noh, 2008). 아름다움이 무엇인지를 아는 인간에게 아름다운 인체란 미의 중심을 차지한다는 신념을 가지게 한다. 따라서 인체에 아름다움을 부여한다는 것은 매우 중요한 의미를 갖는다(Lee, 2007).
현대에 들어 ‘외모지향주의’가 사회 풍조로 대두되면서(Kim et al., 2009), 현대인들에게 있어 ‘외모’는 상대방과의 비교 대상이 되는 동시에 성공적인 대인관계의 필수 불가결한 요소로 작용하게 되었다(Kim, 2017). 이에 따라 사람들은 결점이 있는 자신의 외모를 탈피하여 더 좋은 외모를 가지기 위하여 적극적으로 시간적, 물질적인 투자와 노력을 하고 있으며(Lee & Koh, 2006), 이에 편승한 의학과 미용 산업이 꾸준하게 발전되면서 부작용 등의 위험성은 더 적으나 만족도는 더 높은 방법을 개인적으로 선택하여 외모를 가꾸기에 이르렀다(Jang, 2010).
여성들의 사회적 활동 비율이 높아지면서 이러한 외모 관리에 대한 관심은 더 높아져, 성공적인 자기가치 실현을 위해 메이크업, 성형, 몸매관리 등을 통하여 더 아름다워지고자 하며(Kim, 2016), 또한 미의식은 비단 여성 뿐 아니라 남성들도 예외는 아니어서 더 나은 외모를 위한 관리에 적극적이고 긍정적인 관리태도를 취하고 있다(Kang, 2017). 이러한 미적 욕구를 전문적으로 충족시켜 줄 수 있는 곳으로 병원 내 피부·비만 클리닉 센터와 피부·비만관리실(에스테틱 숍)이 대표적이다(Kim, 2011).
한편, 우리나라의 고도 비만 인구는 2030년에 현재의 2배 수준에 이를 것이라는 전망이고(MOHW, 2021), 비만으로 인한 사회경제적 손실 규모는 최근 10년 사이 2배 이상 증가하여 손실비용이 2016년 약 11조 5천억 원이라고 보고하였다(KHPI, 2020). 또한, 세계보건기구(World health organization, WHO)는 비만을 장기치료가 필요한 질병 21세기 신종 감염병으로 지목하였고(Economic Review, 2019; WHO, 2015), 경제협력개발기구는 세계 주요 경제권에서 비만으로 인한 사회경제적 비용이 심각한 수위에 이른다고 한다(Yunhap news, 2019).
비만은 단순히 체중증가나 외모 문제뿐만 아니라 신체적, 정신적, 사회적 질환 발생의 원인으로 작용하고(Korean Society of Obesity, 2018), 심 뇌혈관질환 및 암에 의한 사망률을 증가시키는 매우 위험한 요소다(Calle et al., 2003; Lord et al., 2002; Zametkin et al., 2004). 최근에는 비만도가 높아질수록 대장암, 직장암, 간암, 담도암, 전립선암, 신장암, 갑상선암, 폐의 소세포암, 림프종, 피부암 등의 발생위험이 높아진다는 사실도 발견하였다(National Cancer Center, 2018). 비만의 예방 대책은 식이조절과 섭취와 소비의 균형에 있다(Kraemer et al., 2004; Martins et al., 2007)고 하지만, 현대인들의 식생활 패턴은 비만을 유발 할 가능성이 높고 섭취와 소비의 균형을 지키기에는 어려움이 많아 전문적인 비만관리의 요구가 필요해진다. 이렇게 비만이 점차 사회 위협요소가 되고 있어서 비만인구 증가를 대비한 정부 차원의 예방 대책(MOHW, 2021)이 마련되고, 이로 인한 비만산업이 향후 급성장하고 산업적 성공기회가 될 수 있을 것이란 전망이다(SERI, 2012).
선행연구에 의하면 피부 비만 관리에 관한 고객선호도와 이용 빈도는 개인 피부미용실과 병원 부설 피부미용실이 가장 많은 것으로 나타났고(Roh, 2015), 기기관리와 수기관리의 병행 요법으로 상호 보완 및 상승작용이 더해져 관리효과의 극대화를 통한 융합솔루션의 개발 연구(Lee, 2016)의 필요성도 대두되었다.
또한, 복부 비만 진단을 위한 구체적인 검사 방법의 연구(Jeon, 2010)와 한방비만프로그램의 치료 효과를 연구한 논문(Kim & Lee, 2001; Lee & Lee, 2001; Lee et al., 2009)들이 지속적으로 보고되고 있고, 체중 감량 경과에 대한 연구(Hwang et al., 2009)들은 있었으나, 아직까지 한의원의 한방비만치료 행태에 초점을 둔 통계연구는 미흡하며, 특히 한방 의료기관 내 미용 요법을 이용한 비만 관리현황과 행태에 대한 연구는 부족한 편이다.
사람들이 비만 관리를 시도한 목적은 연령대 구분 없이 외모상의 이유가 가장 큰 비율을 차지하였고, 다음으로는 건강상의 이유, 자신감의 결여 등이 선행연구 결과로 나타났다. 또한 비만 관리 경험이 있는 대상자가 전체 설문 응답자 중의 80%를 넘는 상황에서 전체의 66.7%가 불만족스럽다고 보고 하였다(Park, 2010).
이러한 추세가 반영되어 미용분야에서는 비만에 관한 연구들이 활발하게 이루어지고 있는데, 비만 감소에 긍정적인 영향을 줄 수 있는 관리 방법과 효과를 분석하거나(Heo & Yoo, 2017; Jeon, 2014; Jung, 2013; Kim, 2005; Park, 2010; Park, 2016; Park & Han, 2016), 비만 해소와 병행한 체형관리에 효과적인 방법에 대한 연구(Choi et al., 2009; Jeong & Kim, 2016), 비만 관리현황 파악과 행태연구(Lee et al., 2012; Park & Park, 2018) 등으로 다양하게 접근하고 있다. 특히 병원 부설 피부미용실은 비만 관리가 의료적 측면이 주를 이루고 있어 개인 피부미용실 간의 고객 유치를 위한 경쟁이 심화 될 것을 예측한 보고(Park & Park, 2018)도 있다.
현재 한의원 비만 클리닉의 발전 속도에 비해 비만해소를 원하는 수요나 시장은 더 빠르게 확대되고 있고 앞으로 비만 관리의 수준과 전문성의 향상이 절실히 필요한 시점에 왔다고 할 수 있다. 하지만 한방 의료기관에서 실제로 시행하는 비만 관리의 수준이나 전문성은 다소 미흡하며, 비만 클리닉의 프로그램 유형을 조사하거나 시행실태를 파악하는 등의 구체적인 연구는 많이 이루어지지 않고 있는 실정이다. 따라서 본 연구에서는 한방 의료기관에서 비만 치료와 미용 요법을 이용한 비만 관리를 효율적으로 활용하는 방안을 제시하는데 그 목적을 두고, 한방 의료기관에서 시행하고 있는 비만 치료현황과 병행하는 미용 요법을 이용한 비만 관리현황을 살펴본 후에 선행 연구된 미용 분야에서의 비만 관리의 효율성에 대한 한의사들의 인식 정도를 파악하고자 하였다.
이에 본 연구가 한방 의료기관의 비만 치료와 미용 분야의 비만 관리가 향후 협업 또는 융합이 가능할 것인지 가늠할 때 기초 자료로 활용되기를 바란다.
II. 내용 및 방법
1. 연구목적
현재 임상에서 널리 행해지고 있는 한의원의 비만 치료법의 종류와 각종 연구에서 밝혀진 치료효과, 미용 요법을 이용한 비만 관리의 종류와 효과들을 살펴본 후에, 한의원에서의 비만 치료현황, 비만 치료와 병행하고 있는 미용 요법의 비만 관리 방법들의 활용 여부, 고객(환자)의 만족도, 향후 활용 의사에 대한 한의사들의 인식 정도를 파악하는 것이 본 연구의 목적이다. 이를 위해 다음의 각 사항들을 조사 분석하고자 한다.
첫째, 한의원의 기본진료에 비만 치료를 추가 시행하면 매출이 증대될 것인가?
둘째, 치료와 미용 분야의 비만 관리를 병행할 경우 고객(환자)의 만족도는 더 높아질 것인가?
셋째, 효과가 검증된 미용 분야 비만 관리 정보를 제공할 경우 치료와 병행하는 비율은 높아질 것인가?
넷째, 비만 치료에 있어 미용 분야 비만 관리에 대한 한의사들의 인식이 긍정적일까?
다섯째, 한의원에서 미용 요법의 비만 관리가 활성화되면 미용학과 학생들의 취업 영역이 넓어질 것인가?
여섯째, 비만 치료와 관리에 있어 한의원과 피부미용실은 상호 영업적 협업 또는 융합 가능성은 있을 것인가?
일곱째, 한의원과 피부미용실의 영업적 협업 또는 융합이 이루어지면 부산, 울산, 경남의 비만 관련 의료산업과 뷰티관광 산업의 활성화에 도움이 될 것인가?
2. 연구대상 및 연구대상자 선정
본 연구에 앞서 비만 치료 및 관리의 일반적 현황을 파악하기 위한 표적 집단 심층면접조사(Focus Group Interview; FGI)를 실시하였고. 한의원에서 비만 치료 경험이 있는 한의사 중 연령대별(30대, 40대, 50대) 3인과 비만 관리를 하고 있는 에스테틱샵 피부미용사 5인을 대상으로 2그룹으로 나누어 심층 면담을 하였다.
한의원에서의 비만 치료 및 관리행태와 관련된 내용을 중심으로 면접시간은 한 그룹에 30분가량 소요되었고, 면접 후 자료 분석을 위해 인터뷰 내용 중 공통적인 특징들을 정리하여 연구자의 연구목적에 맞게 수정·보완하여 설문지를 구성하는 데 사용하였다.
면접조사의 내용은 인구통계학적 사항, 비만 치료와 관리의 일반적 사항, 비만 치료현황과 치료 후 발생하는 현상, 미용 요법의 비만 관리현황과 관리 후 발생하는 현상 등이었다.
연구대상자는 주로 부산, 울산, 경남에 있는 한의원에서 비만치료 및 관리를 담당하는 한의사로 하고, 기타 지역은 SNS(카카오톡)로 URL을 배부할 수 있는 한의사로 선정하였다.
3. 측정 도구의 구성
본 연구자가 준비한 설문자료는 선행연구(Park, 2010; Shin, 2013)를 참조하여 한의원에서의 비만 치료 및 관리행태와 관련된 내용으로 구성하였고, 측정 도구는 인구통계학적 특성 8문항, 비만 치료와 관리의 일반적 사항 23문항, 비만 치료현황과 치료 후 현상 19문항, 미용 요법의 비만 관리현황과 관리 후 현상 18문항, 비만 관리와 치료의 융합 또는 협업에 대한 의향조사 5문항, 총 73문항이고, 설문조사는 총 10분 내외로 소요될 것으로 예상하였다. 설문 구성은 Table 1과 같다.

Configuration of measuring tools
4. 조사방법
본 조사는 영산대학교 생명윤리위원회(IRB)의 심의를 거쳐 승인을 받아 자료 수집을 위한 설문조사를 시행하였다(IRB 승인번호: YSUIRB-202105-HR-088-01).
본 연구의 표본조사 대상자는 한의원에서 비만 치료를 담당하는 한의사로 선정하였고, 본 조사 설문에 앞서 신뢰성을 위해 연구대상자로 선정된 전국의 한의사를 대상으로 2021년 3월 25일부터 4월 15일까지 3주간 SNS(카카오톡)을 통해 URL를 배부하여 사전조사를 실시하였고, 사전조사의 분석결과를 토대로 설문의 문항을 수정·보완하여 최종 설문지를 재구성하였다.
부산, 울산, 경남 및 기타 지역에 위치한 한의원 2200여 군데의 한의원에서 비만 치료를 담당하는 한의사를 상대로 2021년 7월 26일부터 9월 6일까지 6주간 연구에 대한 목적과 취지를 설명하고, SNS(카카오톡)를 통한 URL 배부, QR코드를 생성하고 설문지에 기입하여 우편 발송 후 QR코드로 접속하여 직접 입력, 설문에 대한 답을 답안지 형태에 기입하여 팩스로 전송 혹은 답안을 사진으로 받아 입력하는 방식으로 조사를 시행하였다.
5. 자료수집 및 통계방법
수집된 답변들은 자료정리(Data Cleaning)를 거쳐 불성실한 답변을 제외하고 총 448부를 최종분석 자료로 사용하였으며, 수집된 자료는 SPSS 24.0 프로그램을 이용하여 분석하였다. 분석기법으로는 연구대상자의 일반적 특성을 파악하기 위해 빈도와 백분율을 산출하였으며, 독립성검정, 카이제곱검정(Chi-Squared test), 다중응답분석, 빈도분석을 실시하였다.
III. 이론적 배경
1. 한의원 내 비만 치료법의 종류와 효과 연구
1) 약물요법 및 치료 개괄
한의학에서 비만 치료는 크게 다음과 같이 나눌 수 있다. 비만의 원인이 기허(氣虛), 간기울결(肝氣鬱結), 고량후미(膏粱厚味) 등에 의해 습담(濕痰), 어혈(瘀血)이 축적된 것으로 보고(The Society of Korean Medicine Rehabilitation, 2015), 보기건비(補氣健脾), 화습이수거담(化濕利水去痰), 통부소도(通腑消導), 활혈통락(活血通絡) 등의 치료법을 활용하고 있고, 약선(藥膳)요법, 안마요법, 부항요법, 훈기욕(薰氣浴), 절식요법 등을 이용(Kim et al., 2000)하거나, 이침, 체침, 전기지방분해침, 한약, 기공요법(Hwang et al., 2007) 등으로 치료한다.
사상체질론에서 보면, 에너지 소모 배설의 장기인 심장(心), 폐장(肺), 신장(腎臟)의 기능이 강해서 상대적으로 소모되기 쉬운 체질인 태양인 소음인과 소화흡수 장기인 비장(脾臟), 간장(肝臟)의 기능이 강해서 체중증가가 상대적으로 쉬운 체질인 소양인 태음인이 있는데(Heber, 2004), 사상의학에서는 각 체질에 맞추어 섭생을 조절하고, 적절한 약과 처방을 선택한다면 평소 관리가 가능하다고 하였다(Jo, 2005).
2) 약침(경피침주요법), 매선요법
대한약침학회에 의하면 약침이란 순수 한약재 등에서 추출, 정제, 희석, 혼합 또는 융합한 약액을 침을 놓는 자리(경혈, 경대, 경근, 관절, 각종 강내, 혈맥 등)에 자입, 투입, 매몰하는 한방 치료법을 말한다. 약침을 활용한 비만 연구의 실험실적 및 임상적 연구 동향 고찰에서 비만 개선에 사용되는 약침의 재료 종류는 웅담, 우황, 마황, 부평, 산양산삼, 황금 등이었고, 현재까지 발표된 동물실험, 세포실험, 임상실험 등을 살펴보았을 때, 약침요법을 이용한 국소 비만 치료는 효과적이며 발전 가능성이 높은 비만 치료법(Kim et al., 2011)이라고 하였다. 산삼비만약침과 매선요법을 병행한 복부비만 치료의 임상 효과(Shin, 2013)에서는 부분 비만에 단기간 효과가 있다고 알려져 있는 산삼비만약침과 지방분해 효과를 지속시켜 준다고 알려져 있는 매선요법의 결합이 부분적인 피하지방의 분해에 상당히 효과적이라는 점을 확인할 수 있었고, 부분비만 개선을 위한 매선과 약침의 병행 치료 임상 효과 증례 보고(Chon & Yoo, 2015)는 약침을 복합하여 사용하는 연구 시도였다. 임상의들에게 제공되는 부분비만치료를 위한 산삼비만약침의 임상적 활용방법, 산삼비만약침의 시술 방법 및 임상응용(한방비만학회) 등도 있었다.
3) 전기온열치료와 기타요법
비만 치료에 사용되는 요법으로는 전기온열(저주파 지방분해침, 초음파, 고주파 치료), 약물 주입(메조테라피, 경피침주요법), 마사지 방식(감압치료), 가스 주입(탄소피하주사:카복시) 등이 다양하게 활용되고 있다(Song, 2006). 그 중에서 태음조위탕과 전기침 병행치료의 비만에 대한 효과(Jang et al., 2001)와 체감의이인탕 복용과 전침시술이 체지방감소에 미치는 효과(Kim & Kim, 2002)는 약물요법과 전침을 결합하여 지방을 분해하는 비만치료 연구인데, 연구결과에서 한약단독복용에 비해 전침병행치료가 체지방 감소효과가 높으며 부분비만개선 및 근육량 유지에 보다 효과적이라고 하였다.
4) 기타 비만 관련 연구
기존의 비만 치료 외에 다양한 방법의 연구들도 있는데, 핀다요법은 약재를 광목에 싸서 스팀에 찐 상태로 수기를 하는 수치료요법이며, 부항의 주관법을 이용하여 12 피부 자극, 절식요법, 감로수 절식요법 등이 있었다. 여기서 절식이란 일반적으로 단식이라 알려져 있는 것으로 일정 기간 영양공급을 중지하거나 열량섭취의 제한을 통해 몸속의 노폐물과 독소를 배출하는 해독요법의 한 범주다(Lee & Hong, 2011; The Society of Korean Medicine Rehabilitation, 2015).
이 중에서 흥미로운 것은 여성 환자를 대상으로 한방비만치료 프로그램을 통해 단기간의 체중 감량 경과와 그 관련 인자로 운동에 대한 관리 유무, 연령을 설정하여 그 차이를 비교하였는데 체중 감량 효과가운동프로그램 포함 유무보다 연령의 인자의 영향이 더 큰 것으로 나타났다는 연구였다(Lee et al., 2009). 비만 중재 관련 무작위배정 비교임상연구 보고의 spin 연구(Lee et al., 2017)에서 많은 임상의들이 비만 치료의 새로운 근거를 학술지에 의존하고 있으며 원천자료를 보지 않아 임상 연구에서의 spin은 더욱 위험하다(Schroll et al., 2016 재인용)는 지적과, 연구자료 발표 및 이용의 엄정성이 더욱 요구되고 있다(Sui et al., 2012; Esteghamati et al., 2015 재인용)는 내용은 눈여겨 볼만하다.
2. 미용 요법을 이용한 비만 관리의 종류와 효과 연구
1) 비만 관리현황과 행태
미용요법을 통한 비만 관리현황을 조사한 결과에 따르면, 관리요법은 마사지요법, 기기요법, 열관리요법, 슬리밍제품요법, 운동요법, 행동수정요법 순으로 실시되고 있었고, 마사지요법은 경락마사지, 아로마, 괄사, 스톤, 발, 아유르베타, 타이 마사지 순이었으며. 기기 요법은 고주파기기, 감응전류기기, 초음파 기기 등이 실시되고 있었다. 열관리요법의 종류로는 증기관리가 가장 높게 나타났다(Park, 2010).
2) 경락마사지
부위별 마사지가 중년여성의 호흡 순환기능과 비만 인자 및 면역기능에 미치는 영향(Kim, 2013)에서는 부분 마사지와 전신 마사지를 비교연구 하였고, 수기요법이 여성의 체형균형 및 혈액의 생화학적 지수에 미치는 영향(Shin, 2011)에서는 스웨디시 마사지(Swedish Massage)와 니탸 라크루아(Nitya Lacroix)의 마사지 방법을 기본으로 하고 경락, 경혈, 지압 및 카이로프락틱 등 다양한 수기요법을 시행하였다.
경락마사지를 이용한 방법연구에 대하여 메타분석을 활용한 경락마사지의 효과 연구가 이루어졌는데 생리적 변인군의 비만 조절 관련 변인은 모두 신뢰구간에서 유의한 효과를 갖는 것으로 나타났다. 그 중 가장 큰 효과 크기를 보인 것은 복부지방률이었으며, 그다음 체질량지수, 체중, 복부비만률, 체지방량, 체지방률, 제지방량 순으로 나타났다(Jeong, 2013).
3) 수기(마사지)요법
여러 형태의 수기요법에 대한 연구로서는, 수기 미용 성형요법 마사지, 슬리밍 크림을 이용한 마사지, 골근 마사지, 온열마사지, MNIT수기법 등이 있는데, MNIT수기법이란 근육에너지 기법을 응용한 마사지기법이다. 이 외에 림프 드레나쥐, 추나마사지와 스웨디시 마사지, 추나 미용 등도 있는데 추나라는 한방치료기술을 미용에 접목한 것으로 향후 주목할 필요가 있을 것으로 사료된다. 이러한 수기요법이 비만 관리에 미치는 효과에 대한 메타분석에서 수기요법이 비만조절변인군인 체질량지수(BMI), 복부비만율(WHR), 제지방량, 체수분량, 체중, 체지방량, 체지방률에 효과적임을 입증하였다(Park & Han, 2016).
4) 아로마(마사지)요법
아로마를 이용한 비만 관리가 증가하는 상황에서 아로마 마사지에 대한 체계적 고찰(Lee et al., 2012)에서 메타분석 결과 아로마 마사지가 비만에 효과적이라는 결과물이 지배적이라는 연구결과가 나왔다. 또한 아로마테라피의 비만 관리효과의 메타분석(Jeon & Woo, 2014)에서 비만관리에 주로 사용한 아로마는 쥬니퍼, 사이프레스, 그레이프후르츠 등 이었고, 캐리어오일은 호호바와 아몬드를 주로 사용한 것으로 나타났다. 아로마 향기 요법 관련 변인에 대한 메타분석(Park, 2016), 아로마요법의 비만 관리효과에 대한 메타분석(Heo & Yoo, 2017) 연구의 결과를 종합하면 아로마 마사지요법은 체중, 체질량지수, 체지방률, 허리둘레, 복부 둘레 감소에 효과가 있으며, 총콜레스테롤과 저밀도 지단백 콜레스테롤 조절에도 효과가 있는 것으로 나타났다.
분석 검증연구로는 아로마테라피의 생리적, 신체적, 심리적 치유 효과에 대한 메타분석(Jeon, 2014)이 있었는데, 적용방법별 효과 크기는 흡입법>마사지법>기타방법 순으로 나타났고 일반인을 대상으로 비만 관리, 심리상담, 건강관리 등 다양한 목적의 미용적·심리적 아로마테라피 프로그램의 효율적 선택과 적용방법을 제시한 것으로 파악된다.
5) 미용기기요법
기기를 이용한 비만 관리법으로는, 경락마사지와 엔더몰로지, 진공음압롤러 기기 마사지, 초음파와 DITI를 이용한 진공음압롤러 기기마사지 등이 있었는데 진공음압롤러 기기는 엔더몰로지와 같은 것이다. 고주파기를 이용한 복합 프로그램과 초음파를 이용한 비만관리법의 연구, 캐비테이션 초음파 관리 등도 있었는데, 초음파 캐비테이션 현상이란 강한 초음파 조사 조건에서 매질(주로 유체) 내에서 미세 기포를 발생시키고, 천이시키는 물리적 현상을 의미한다(Noh et al., 2012). 체외충격파기기요법과 수기요법을 이용한 것, 수정보석온열요법, 온열스톤 마사지 등도 있다.
IV. 결과 및 고찰
1. 한의원에서의 비만치료 및 관리 행태 조사 분석 및 고찰
1) 비만치료와 관리를 모두 하는 곳은 15.8%, 비만치료는 하지만 관리는 하지 않는 곳 48.2%, 비만치료 및 관리를 하지 않는 곳 35.9%로, 미용요법의 비만관리 프로그램을 실시하지 않는 곳이 전체의 84.2%이었다. 내용은 Table 2와 같다.

General obesity treatment and obesity management
비만치료만 하는 곳과 치료와 관리를 병행하는 곳 중에서 원장이 직접 시행하는 곳은 67.2%이었고, 관리실의 규모가 10평 미만인 곳이 73.2%이었다. 월 내원 고객(환자)수는 74.2%가 10명 미만이었고, 월 매출액이 200만원 미만인 곳이 57.8%, 내원 환자의 여성 비율이 80% 이상이 66.6%이었다. 내용은 Table 3와 같다.

General obesity treatment and obesity management
2) 비만치료 및 관리를 하지 않는 경우 향후 시행할 의사가 없는 곳이 65.8%로 시행할 의사가 있는 곳보다 많았고, 향후 비만치료를 시행하였을 경우 매출증가에 대한 예상은 증가하지 않을 것으로 답한 곳이 58.4%로 매출이 증가할 것이라는 응답보다 많았다. 예상하는 매출 증가 비율은 현재 매출 대비 증가하지 않거나 10% 이내일 것이라는 응답이 29.2%, 10~20% 증가가 50.9%로 가장 많았고 20% 이상 증가를 예상하는 응답은 19.9%이었다. 내용은 Table 4와 같다.

If obesity is not treated and managed
3) 비만치료를 하지 않는 이유는 주된 치료분야가 아닌 경우가 79.8%로 가장 많았고, 비만관리를 하지 않는 이유는 필요성을 못 느껴서, 정보가 부족해서, 공간이 협소한 문제 순이었다. 내용은 Table 5와 같다.

Reasons not to treat obesity (multiple responses)
비만치료는 하지만 관리는 하지 않는 경우 향후 시행할 의사는 72.4%가 “없다”고 답하였고, 비만관리를 시행한다면 매출이 오를 것이라는 응답은 보통으로 응답한 경우를 포함해서 74.5%가 매출이 증가할 것이라고 예상하였다. 매출 증가 비율은 10~20% 증가 39.3%, 20% 이상 증가 37.9%이었다. 세부내용은 Table 6과 같다.

If obesity is not controlled
4) 한의원에서 시행하는 비만치료법의 종류를 분석한 결과, 287곳의 비만 치료 한의원 중 약물요법은 277(96.5%)곳에서 시행하고 있었고, 전침요법(지방분해침), 약침요법, 한방 물리치료기, 매선요법, 해독요법, 추나요법 순으로 나타났다. 내용은 Table 7과 같다.

Types of obesity treatment (multiple responses)
약물요법에 사용하는 한약은 주로 한의원내 탕전실에서 자가 처방을 사용하는 경우가 61.7%로 가장 많았고, 원외 탕전원의 약속 처방, 원외 탕전원에서 자가 처방, 한방의료보험약 순이었다. 한방 물리치료요법에 사용하는 기기로는 중저주파 23.1%로 가장 많았고, 간섭파, 고주파, 메조테라피, 카복시, 초음파 순이었다. 내용은 Table 8, 9와 같다.

Preparation of herbal medicine (multiple responses)

Types of oriental physical therapy devices used (multiple responses)
5) 비만 치료 완료 후 고객(환자)의 54.4%가 만족하는 것으로 나타났고, 보통 42.5%를 포함하면 만족도는 높았다. 비만 치료로 인한 매출의 증가 비율은 치료 시행 전 대비 10~20% 증가한 곳이 44.9%로 가장 높았고, 전체 응답의 약 90%가 매출이 증가한 것으로 나타났다. 내용은 Table 10과 같다.

What happens after completing obesity treatment
고객(환자)가 선호하는 비만 치료방법은 약물요법이 64.3%로 가장 높았고, 약침요법, 전침요법, 한방 물리치료기, 매선요법과 해독요법, 추나요법 순이었다. 내용은 Table 11과 같다.

Patient's preferred method (duplicate questions)
6) 한의원에서 시행하는 비만 관리 프로그램의 종류는 식이요법이 27.1%로 가장 많았고, 수기요법, 운동요법, 기기요법, 행동수정요법, 온열관리요법, 슬리밍제품 순이었다. 내용은 Table 12와 같다.

Types of obesity management programs (multiple responses)
수기요법의 종류는 경락마사지 29.4%, 림프마사지 27.5%, 아로마마사지 21.1% 등이었고, 미용기기요법에 사용하는 것은 고주파 마사지기 30.7%가 가장 많았고, 부항요법, 중저주파 전류기기, 이온토 테라피 순이었다. 고객(환자)이 선호하는 관리요법은 수기요법이 34.5%로 가장 많았고, 식이요법, 운동요법, 행동수정요법, 기기요법 순이었다. 내용은 Table 13, 14, 15와 같다.

Types of manual therapy (multiple responses)
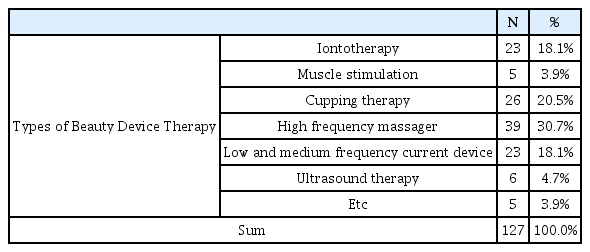
Types of beauty device therapy

Patient preferences during obesity management (multiple responses)
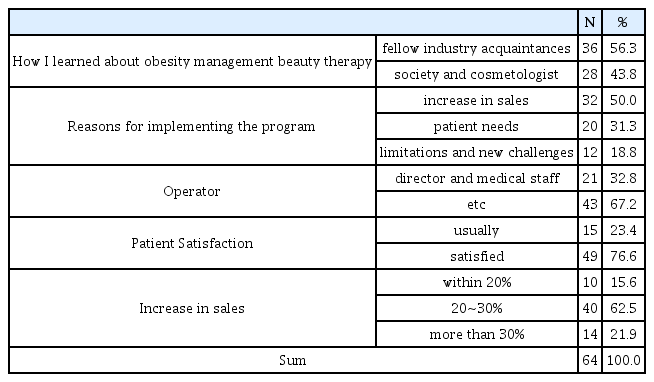
7) 비만치료를 하는 한의사가 미용요법의 비만관리를 알게 된 경로는 동종 업계 지인을 통해서, 학회 및 미용종사자를 통해서였다. 관리 프로그램을 시행하게 된 이유는 매출 증가를 위해서, 환자의 요구, 치료의 한계성 때문과 새로운 진료 영역에 대한 도전 욕구 순이었다. 비만 치료와 관리(미용요법) 프로그램을 병행했을 때, 비만치료만 단독으로 했을 때보다 매출증가는 20~30% 증가 62.5%, 30% 이상 증가 21.9%, 20% 이내 증가 15.6%로 비만관리를 병행하는 것이 매출 증가에 영향을 미쳤음을 알 수 있었다. 내용은 Table 16과 같다.
What happens after obesity management is completed
비만 관리 프로그램 중 효과가 좋은 것부터 순서대로 나열한 결과는 수기요법, 식이요법, 기기요법, 운동요법 순이었다. 내용은 Table 17과 같다.

The most effective treatment for obesity management programs
8) 한의사에게 미용분야에서 검증된 효과적인 비만 관리법 정보를 제공한다면 현재 시행하고 있는 비만 치료와 병행할 의사가 “있다”는 62.7%이었고, 향후 상호간의 융합 및 협업 가능성에 대해서는 70.5%이 가능성이 “있다”고 답했다. 한의원에서 비만 관리를 시행하면 미용분야에 재학 중인 학생들의 현장 실습 기회와 취업에 기여할 수 있겠는가에 대해서는 62.5%가 “그렇다”고 답했으며, 상호 융합 또는 협업이 이루어졌을 때 미용 산업과 한방의료 관광산업의 매출이 증가할 것으로 생각하는가에 대해서는 70.8%가 “그렇다”고 답했다. 상호 융합 또는 협업이 이루어졌을 때 내·외국인의 한방 의료산업 및 미용 관광 산업의 선호도 상승과 활성화에 도움이 될 것인가에 대한 생각은 71.9%가 “그렇다”고 답했다. 상세내용은 Table 18과 같다.

Convergence and collaboration between cosmetic therapy obesity management and oriental medicine obesity treatment
2. 인구통계학적 특성에 따른 비만 치료 및 비만 관리의 일반적 사항에 대한 조사 분석 및 고찰
1) 비만치료를 하는 경우 매출 증가에 대한 조사 분석 및 고찰
한의원에서 기존의 진료과목에 비만치료를 추가하면 매출이 증가한다는 것을 알 수 있었고, 여자 한의사, 임상경력이 20년에 가까울수록, 월 매출이 많을수록 비만치료로 인한 매출증가가 높음을 알 수 있었다. 내용은 Table 19, 20, 21과 같다.

Obesity treatment and management and sales by gender

Obesity treatment and management and sales by clinical career

Obesity treatment and management and sales by monthly income
2) 비만치료와 미용 분야의 비만 관리의 고객(환자) 만족도에 대한 조사 분석 및 고찰
환자의 만족도 조사에서는, 월수입이 많을수록 고객(환자)의 치료만족도가 높았다. 내용은 Table 22와 같다.

Satisfaction after completion of treatment by monthly income
비만관리를 하는 경우에, 임상경력이 20년 미만일수록, 월수입이 높을수록, 재방문자가 많은 한의원일수록 고객(환자) 만족도가 높다는 것을 알 수 있었다. 하지만 비만치료에 대한 고객(환자) 만족도와 비만관리를 추가 시행한 만족도 간의 비교 검증은 불가능하였다. 세부 내용은 Table 23, 24와 같다.

Satisfaction after completion of omanagement by clinical career

Satisfaction after completion of management by monthly income
3) 효과가 검증된 미용 분야 비만관리 정보를 제공할 경우 치료와 병행할 의사에 대한 조사 분석 및 고찰
남자 한의사, 나이가 들수록, 도시규모가 큰 곳보다는 작을수록, 월수입이 많을수록 비만관리의 시행의사가 높은 것을 알 수 있었고, 한의사들의 비만관리에 대한 요구도가 높다는 것을 알 수 있었다. 세부 내용은 Table 25, 26, 27, 28과 같다.

Thoughts on obesity treatment and management according to gender (If obesity is not controlled)

Thoughts on obesity treatment and management according to clinical career (If obesity is not treated and managed)

Thoughts on obesity treatment and obesity management according to location (If obesity is not controlled)

Thoughts on obesity treatment and obesity management according to monthly income (If obesity is not treated and managed)
4) 비만 치료에 있어 미용 분야 비만 관리에 대한 인식이 긍정적으로 변할 것이라는 것에 대한 조사 분석 및 고찰
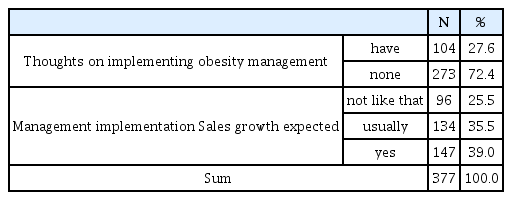
아직까지는 한의사들이 미용분야 비만관리에 대한 시행의사가 적고 임상에서 활용하는 비율이 낮아 비만관리에 대한 인식이 긍정적이지 않았지만, 앞으로 비만관리 시행의사가 있는지 분석결과 의사가 있다가 104곳(27.6%)으로 나타나 향후 한의사들의 비만관리에 대한 인식의 변화를 연구를 통해 관찰해 볼 필요가 있을 것으로 사료된다. 내용은 Table 29, 30와 같다.

Reasons for not managing obesity (multiple responses)
If obesity is not controlled
5) 미용과 한의학적 비만 협업에 대한 조사 분석 및 고찰
비만관리가 활성화되면 한의원의 상황에 따라 변수는 있겠으나 미용학과 학생들의 취업 영역은 전반적으로 넓어질 것이라는 것을 추측할 수 있었다. 또한 한의원에서의 비만 치료와 피부미용관리실의 비만관리의 상호 영업적 협업 또는 융합 가능성은 높았고, 임상경력이 많을수록, 월수입이 낮을수록 가능성이 높다고 보았다는 것은 시사하는 바가 있었다. 내용은 Table 31, 32와 같다.

Collaboration with beauty and oriental medicine obesity treatment according to clinical career

Collaboration with beauty and oriental medicine obesity treatment according to monthly income
미용업과 한의원이 상호 융합 또는 협업이 이루어졌을 때 미용산업과 한방의료 관광산업의 매출이 증가할 것으로 생각하는가에 대해서 70.8%가 그렇다고 답했고, 내·외국인의 한방의료산업 및 미용 관광산업의 선호도 상승과 활성화에 도움이 될 것인가에 대해서는 가능성이 높아 비만 관련 의료산업과 뷰티 관광산업의 활성화에 도움이 될 것으로 사료된다. 내용은 Table 33과 같다.

Convergence and collaboration between cosmetic therapy obesity management and oriental medicine obesity treatment
V. 결 론
본 연구는 한의원에서 비만치료를 위해 시행하고 있는 치료 현황과 미용요법을 이용한 비만관리 현황을 조사한 것을 토대 로, 한의계의 비만 치료와 미용 분야의 비만 관리가 향후 협업 또는 융합이 가능할 것인지 가늠해보는 자료로 활용하는 데 목 적이 있으며, 이를 위해 비만 치료와 관리의 일반적 사항, 비만 치료 현황과 치료 후 현상, 미용요법의 비만관리 현황과 관리 후 현상, 비만관리와 치료의 융합 또는 협업에 대한 의향 등을 중심으로 분석을 실시하였고 결과는 다음과 같다.
첫째, 한의원에서 진료과목에 비만 치료를 추가했을 때 매출이 증가할 것인가? 에 대한 검증 결과, 진료과목에 비만치료를 추가하였을 때 실제 매출이 증가한 곳이 전체 응답의 90%가 넘었고, 여자 한의사, 임상경력이 20년에 가까울수록, 월 매출이 많은 곳일수록 비만치료로 인한 매출증가가 높았음을 알 수 있었다. 또한 비만관리 프로그램을 병행했을 때가 비만치료만 단독으로 했을 때보다 매출이 증가한 것으로 나타나, 현재 비만치료를 하지 않는 한의원일수록 비만치료를 시행하는 것이 월매출 상승에 도움이 될 것임을 알 수 있었고, 비만관리를 병행하는 것이 매출 상승에 더 도움이 될 것임을 알 수 있었다.
둘째, 비만치료와 미용 분야의 비만관리를 병행할 경우 고객(환자)의 만족도는 더 높아질 것인가? 에 대한 검증 결과, 한의원의 월수입이 많은 곳일수록 고객(환자)의 치료만족도가 높았고, 비만관리를 하는 경우에, 임상경력이 20년 미만일수록, 재방문자가 많은 한의원일수록 고객(환자) 만족도가 높았다는 것을 알 수 있었다. 하지만 본 연구 결과에서는 비만치료에 대한 고객(환자) 만족도와 비만관리를 추가 시행한 만족도 간의 비교검증이 불가능하여, 비만치료와 미용 분야의 비만 관리를 병행할 경우 고객(환자)의 만족도는 더 높아질 것인가? 에 대한 검증은 불가하였다.
셋째, 효과가 검증된 미용 분야 비만관리 정보를 제공할 경우 치료와 병행하는 비율이 높아질 것인가? 에 대한 검증 결과, 남자 한의사, 한의사의 나이가 들수록, 도시규모가 큰 곳보다는 작을수록, 월수입이 많은 한의원일수록 비만관리 시행의사가 높다는 것을 알 수 있었고, 한의사들의 비만관리에 대한 요구도 또한 높다는 것을 알 수 있었다.
넷째, 비만 치료에 있어 미용 분야 비만 관리에 대한 한의사들의 인식이 긍정적일 것인가? 에 대한 검증 결과, 아직까지는 한의사들이 미용분야 비만관리에 대한 시행의사가 적고 임상에서 활용하는 비율이 낮아 비만관리에 대한 인식이 긍정적이지 않았지만, 앞으로 비만관리 시행의사가 있는지 분석결과 의사가 “있다”가 104곳(27.6%)으로 나타나 향후 한의사들의 비만관리에 대한 인식의 변화를 후속연구를 통해 관찰해 볼 필요가 있을 것으로 사료된다.
다섯째, 한의원에서 미용 요법의 비만 관리가 활성화되면 미용학과 학생들의 취업 영역이 넓어질 것인가? 에 대한 검증 결과, 비만관리가 활성화되면 한의원의 상황에 따라 변수는 있겠으나 미용분야 재학생들의 현장실습 기회와 취업에 기여할 수 있다가 전체 응답의 62.5%로 미용학과 학생들의 취업 영역은 전반적으로 넓어질 것임을 알 수 있었다.
여섯째, 한의원에서의 비만 치료와 피부미용관리실의 비만 관리의 상호 영업적 협업 또는 융합 가능성은 있을 것인가? 에 대한 검증 결과, 전체 응답의 70.5%가 가능성이 “있다”고 답했다. 또한 임상경력이 많은 곳일수록, 월매출이 낮을수록 협업과 융합가능성이 높다고 응답한 것은 시사하는 바가 있었다.
일곱째, 한의원과 피부미용실의 영업적 협업 또는 융합이 이루어지면 부산, 울산, 경남의 비만 관련 의료산업과 뷰티관광 산업의 활성화에 도움이 될 것인가? 에 대한 검증 결과, 매출 증가에 대해서는 70.8%가 “그렇다”고 답했고, 내·외국인의 한방 의료산업 및 미용 관광산업의 선호도 상승과 활성화에 도움이 될 것인가에는 71.9%가 “그렇다”고 답하였다. 이것은 한의계와 미용업계 상호간 융합 또는 협업이 이루어지면 미용 산업과 한방의료 관광산업의 매출 증가와 활성화 가능성을 짐작할 수 있는 기초가 될 것으로 사료된다. 따라서 비만 관련 의료산업과 뷰티관광산업의 활성화에 도움이 될 것임을 알 수 있었다.
본 연구의 분석결과를 통하여 시사하는 내용은 비만치료를 시행하고 있는 한의원은 의료서비스 측면에서 환자에게 높은 만족감을 주었고, 한의원 매출 상승으로 인해 경영에 도움이 되었을 것이라는 점이다. 선행 연구에서 비만관리를 하는 피부미용관리실의 다양한 프로그램 활용이 고객의 만족도를 상승시키고 매출상승에 도움이 되었음을 볼 때, 한의원도 보다 적극적으로 비만치료에 도전하고 더불어 비만관리도 병행한다면, 현재 의료시장의 여러 어려움들을 보다 효과적으로 극복할 수 있을 것이고, 또한 향후 비만인구의 증가에 따른 환자들의 요구에 대응하는 준비가 되어 있지 않은 곳과 차별화가 이루어질 것이다. 기존의 한의원들이 가진 세부적인 비만치료 및 관리 행태들을 실증적으로 분석하여 현실을 보여줌으로서, 한의계의 비만에 대한 치료 접근과 미용업계의 비만관리의 효과가 병행 되어질 때 새로운 비만시장을 개척할 근거를 마련할 수 있을 것이며, 더 나은 후속연구들이 나오는 계기가 될 수 있을것이다.